AI Agents and the Distributed Intelligence Mesh
· Dr. Ramy Azzam
Artificial intelligence in healthcare (yes, again) is entering a more grounded and mature phase. The most meaningful progress no longer comes from distant frontier models that promise everything at once, but from practical AI agents that work quietly inside clinics, across private cloud environments, and within enterprise platforms that hold the entire system together. What is emerging is a layered ecosystem where different types of agents live in the places where they are most effective.
This shift did not become clear to me overnight. It unfolded through experimentation, frustration, and eventually a realisation that architecture matters just as much as intelligence.
The Experiment That Taught Me About Agents
My journey began a few months ago with a weekend project I called the LLM Harmonizer. I believed the best way to improve AI reasoning was to combine the perspectives of several models. In a sense, it was my first real attempt at building a multi-agent system. A prompt would go out to multiple models, each acting as its own reasoning agent. A judge agent then compared their answers, resolved contradictions, and produced a refined synthesis.
I was curious to assess the cost-effectiveness. Each request triggered a cascade of cloud activity, and even the simplest tasks became expensive. It was a moment of clarity. Intelligence is not the problem. Placement was.
That realisation stayed with me as I looked at my own workflow. And I believe everyone should. For someone like me, on the neurodivergence spectrum, I relied on AI for structure, organisation, and clarity far more than creativity or knowledge. Creativity happened away from the screen, mostly while I am in the shower. Knowledge lived in my training and experience. The AI agent I needed most was the one that organised, not the one that thought for me.
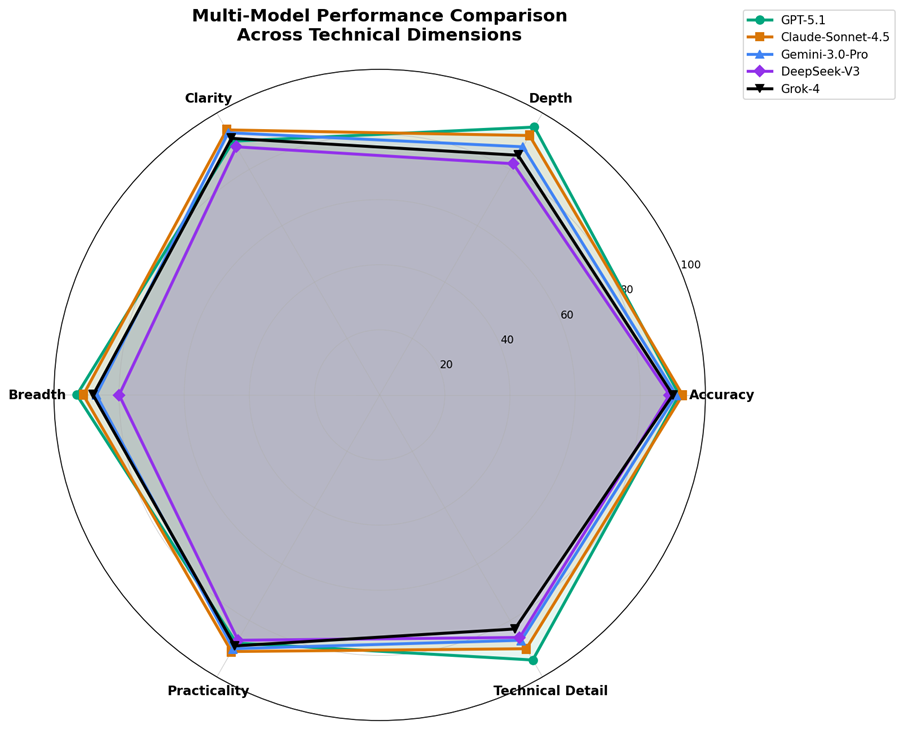
Agreeability analyses required even more tokens
As open source and smaller foundational models began surfacing, I began experimenting with them locally. My modest workstation became a small test environment for building prototypes, drafting, summarising, structuring, and tidying text all happened privately and instantly. It worked so well that I began thinking beyond the individual workstation.
What if every clinic inside a hospital could run its own local agents? After all, hospitals already operate this way in other domains. Imaging servers, EHR systems, departmental applications, and caches of clinical data are already distributed. Agents could fit naturally into that fabric.
The Distributed Clinic Intelligence Mesh
This led me to imagine what I now call the Distributed Intelligence Mesh (DIM).
The inspiration came from patterns we've seen work elsewhere.
? BitTorrent proved intelligence could live at the edges without central servers.
? Between 2007 and 2012, PlayStation 3 owners saw messages that their consoles were contributing to Folding@home, simulating protein folding for disease research. Millions of game consoles, coordinated globally, achieved petaflop scale computing.
? Blockchain showed us distributed consensus: every transaction logged immutably, validated by multiple nodes, governed without centralized control.
In DIM, each clinic runs its own small language model as a local agent, handling documentation, structured data transformation, guideline retrieval, and patient instructions. These agents work close to clinicians, without depending on external networks.
Across the organization, local agents form a coordinated mesh. Like BitTorrent, they share improvements, refinements, and adapters without transferring patient data. They learn from internal patterns without those patterns leaving organizational boundaries. Rare clinical scenarios discovered in one clinic benefit others. The mesh prioritizes rare pieces of clinical knowledge, just as BitTorrent prioritizes rare file chunks.
Above them, private cloud agents oversee trends across clinics, ensure consistency, and manage shared components. They validate updates before propagation, maintaining integrity like blockchain's consensus layer. Every model update gets logged immutably.
At the enterprise level, cloud platforms coordinate population level intelligence, governance, integration, and auditability. But critically, intelligence flows from clinic upward, not enterprise downward.
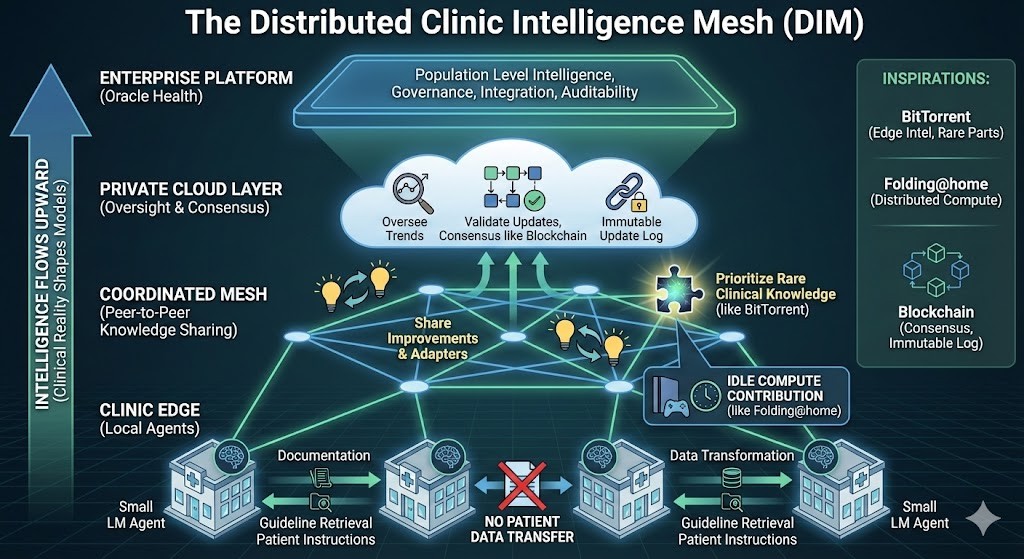
Impressive infographic generated by Gemini 3
The result is an ecosystem where each agent type lives where it is naturally most effective. During off peak hours, clinics contribute idle compute to train shared components, just as PS3 owners contributed to research while sleeping. The mesh enforces privacy through smart contracts. If one node fails, others continue. No single point of failure, no vendor lock in.
The intelligence grows from the edges inward. Clinical reality shapes the models, not corporate assumptions. Every clinic contributes to and benefits from collective capability.
A Hybrid Agent Strategy for a Hybrid AI World
Once you see it this way, the parallel becomes obvious. A hybrid AI deployment strategy naturally supports a hybrid agent strategy. Local models allow for local agents. Private cloud models allow for organisational agents. Enterprise cloud environments allow for enterprise agents.
Each layer mirrors the other. Agents at the edge are fast, private, and responsive. Agents in the private cloud coordinate and maintain coherence across clinics. Agents in the enterprise cloud deliver scale, governance, and integration.
Healthcare already works this way. It has always been a system of distributed roles and specialised functions. AI agents simply map onto a pattern that clinicians and administrators already understand.
AI in healthcare will be agent first. Small agents in clinics will handle the immediate demands and workflow support. Collaborative agents in the private cloud will connect insights across departments. Enterprise agents will provide governance, oversight, and intelligence at scale.
This is not a theoretical future. The components already exist. The architecture is emerging. And the need is immediate.
 If you are designing a healthcare AI strategy, the first question to ask is simple: where should each type of agent truly live? Some agents belong at the clinic edge, close to clinicians and patients. Some belong in the private cloud, coordinating intelligence across departments. And some require the scale and governance of enterprise cloud platforms.
If you are designing a healthcare AI strategy, the first question to ask is simple: where should each type of agent truly live? Some agents belong at the clinic edge, close to clinicians and patients. Some belong in the private cloud, coordinating intelligence across departments. And some require the scale and governance of enterprise cloud platforms.
The organisations that recognise this early will build systems that are faster, safer, and more resilient. They will avoid the trap of over-centralisation while still benefiting from enterprise scale intelligence.
The next productivity curve in healthcare will not come from a single system doing everything. It will come from networks of agents working in harmony across the healthcare environment.