See one. Do one. Teach one. Speak one. Action in a noisy century
· Dr. Ramy Azzam

I remember a dawn surgery round in the oncology center in Egypt back in 2009. The first case was a right hemicolectomy for colon cancer. The senior resident moved with steady economy, narrating each plane as he lifted the ileocolic pedicle, tied the vessels, and freed the hepatic flexure. He talked us through the landmarks as if he were giving a guided tour of living anatomy. Then he paused, looked at me, and asked if I was ready. I took the needle driver and, under his calm voice, closed the mesenteric defect and then stitched the enterotomy after a side to side stapled anastomosis. The theatre felt smaller and louder all at once.
By the second case I was the one explaining orientation and the first stitch to a junior who had been watching me with the same mix of focus and fear. Three short verbs carried the entire arc.
See one. Do one. Teach one.
The classic triad works because it compresses education into motion. You watch with intent, you try with supervision, you explain to confirm understanding. The moment you teach someone else, your own thinking sharpens. No learning management system has ever replaced the shock of being asked to explain a knot while your hands are still shaking from tying it.
Then the world accelerated. Patients arrive with printouts and short videos. New models generate passable drafts of clinical advice. Systems promise transformation and often deliver confusion. The temptation is to replace action with talk. More committees, more announcements, more branding around pilots that never leave the dock. In healthcare that habit has a cost measured in missed care, delayed adoption, and quiet attrition of trust.
The antidote is not nostalgia. It is a modern reading of the triad that still honors speed and safety.
I add one verb that fits our century. Speak one.
Not performative speaking. Not grandstanding. Speak as a duty to share the results of what we tried, good and bad, in plain language.
See one, do one, teach one, speak one.
Then repeat with shorter cycles and better evidence.
See one, with deliberate curiosity
Early in my work with Mubadala I shadowed tele endo consults for days. The setup could not be less glamorous. A laptop on a trolley, a patient who leaned forward to catch every word, a nurse who nudged the camera a few millimetres. Yet those sessions were full of clues you will never find in a slide deck. A cough that interrupted a key instruction. A light glare that made the clinician squint. A moment of silence that signaled uncertainty. Seeing is not passive. It is a form of data collection that respects context.
Seeing also scales when you watch more than screens. Bring frontline nurses into discovery. Invite a registrar to narrate what they are thinking while they click. Ask a patient to show you how they hold the phone during a remote exam. These small acts of careful observation often reveal the easiest fixes. Sometimes the answer is a five minute tip sheet rather than a new platform.
Do one, with small scopes and real outcomes
Doing is where reputations are made. It is also where timid leaders hide behind endless pilots. My rule is simple. Define the smallest test that can still deliver a real decision and a visible outcome. In a remote monitoring program I worked on for hypertension we focused on one ward for thirty days. Our measures were simple. Escalations averted, nursing minutes saved, and a short patient note about clarity of instruction. The small scope kept risk manageable and let us iterate three times before any executive noticed a budget line.
Doing well requires psychological safety. In a theatre, a junior who fumbles a knot must still feel safe enough to say they are stuck. In a startup the intern who catches a privacy flaw at two in the morning needs permission to call the engineer without fear. Our rule of thumb in postmortems is constant. One improvement commitment, one thank you for the person who raised the flag. That culture keeps the middle verb alive.
Teach one, as diffusion not performance
Inside CIGMA, our mental health platform for gamers, the WaveMaker program extends the same logic. A psychology student hosts a discussion about healthy coping strategies inside our community spaces, then trains the next moderator. Each person documents what worked, what flopped, and one thing they would try next week. The recipe spreads without the bureaucracy of a curriculum committee.

Simulation and safety before scale
If the old model looked like see one, do one, teach one, today we add simulate one between see and do. We drill knotted loops on foam pads before we touch skin. We run tabletop exercises for data incidents before we face a live breach. We dry run a chatbot through difficult scenarios before it meets a real person in distress. The point is not to slow down. It is to fail safely and to fail early.
Inside my consultancy we push systems in sandboxes. We stress test prompts, seed edge cases, and collect traces that show how an assistant steers a risky question back toward safety. We use those traces as evidence in our governance files.
The quiet payoff is trust.
When a regulator or a client asks how we know a system behaves, we show the receipts.
Evidence frameworks keep us honest
Agility without evidence becomes churn. Evidence without agility becomes theatre. The way through is to make frameworks a habit rather than a seminar topic.
I use RE AIM as a weekly scorecard. Reach is who touched the new thing and who did not. Effectiveness is the outcome that actually moved, whether it is symptom scores, error rates, or response time. Adoption is which clinicians or ambassadors used the thing without being nagged. Implementation is the friction you can point to, minutes lost, calls missed, help desk notes. Maintenance is what stayed useful after the first week when the novelty wore off. A one page RE AIM brief turns a pilot into a decision.
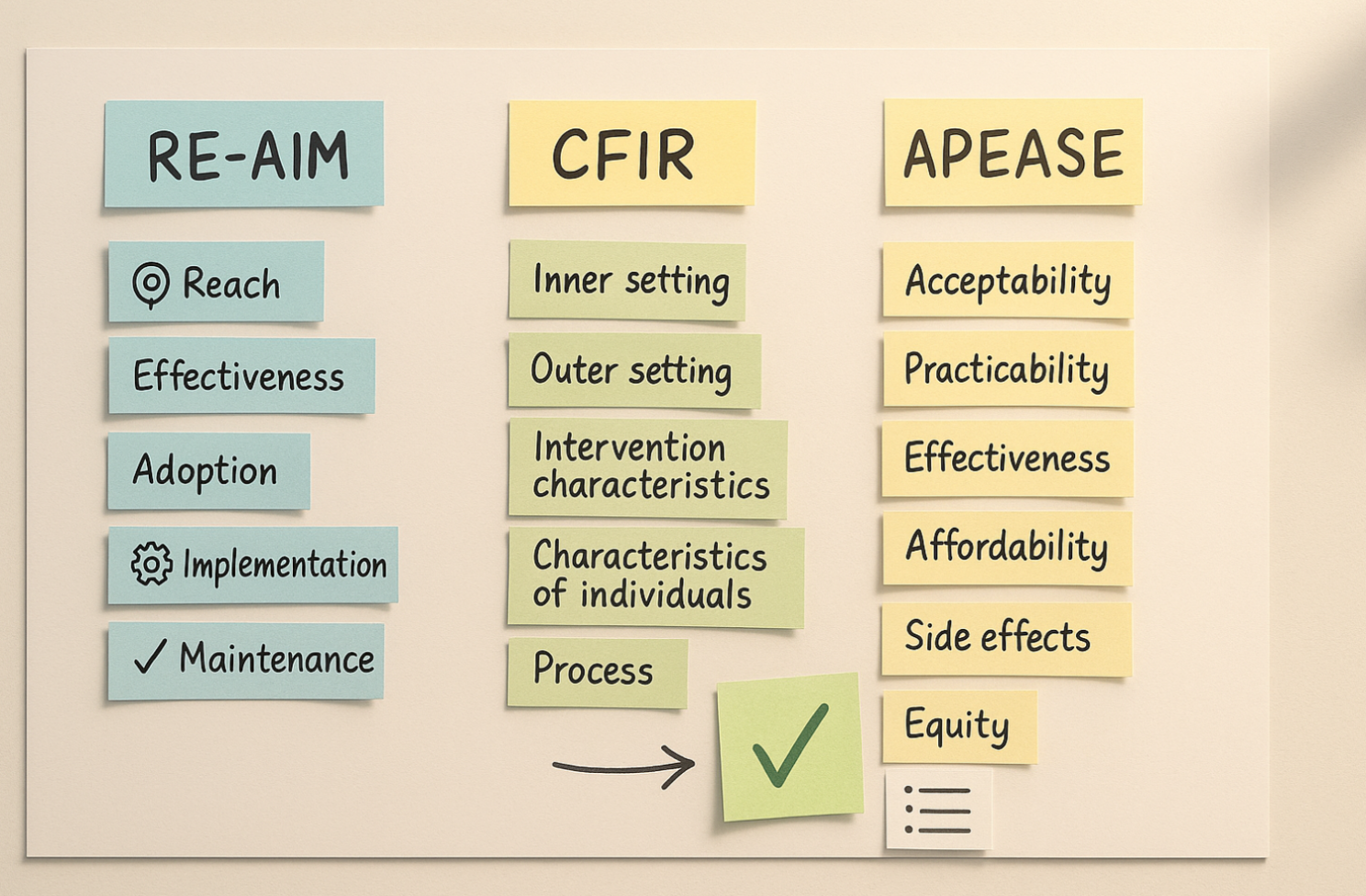
I lean on CFIR when a change feels sticky. Map the determinants. Inner setting culture and incentives. Outer setting constraints like policy, payers, or platform limits. Characteristics of the intervention. Beliefs and skills of the people involved. The process you are actually using, not the one you drew on a whiteboard. Once the determinants are on paper, three change ideas usually present themselves, each with a measure that will tell you if you are moving.
For tough choices between two good options, APEASE brings sobriety. Acceptability for users and staff, practicability with the people and tools you have, effectiveness with a simple outcome you can measure, affordability in plain numbers, possible side effects including risk and harm, and equity for groups that usually get left behind. Write a short decision memo that shows the trade offs and commit to the smallest viable option. That memo is more valuable than another meeting.
Lessons from the boardroom
The triad maps directly to executive work. When I guided a regional network on readiness for AI management, we began with a hard look at reality. That was our see. We lined up all the so called AI use cases and asked which ones had monitoring, drift alerts, and clear owners. Many did not. The do phase was a corrective plan with names and dates, not a wish list. The teach phase came when compliance officers taught peers in sister hospitals how to set up the same guardrails. The speak phase was a quarterly update to the board and to clinical leaders that showed what changed and what did not. No slogans, no confetti, just visible progress.
Where the model fails and how to avoid it
There are traps that can swallow a year. Pilot creep, where projects grow to fit the largest room on the floor. Teaching that becomes a monologue rather than a hand off. Speaking that becomes performance rather than service.
The worst trap is confusing noise for action.
My guardrails are simple. Keep scopes small. Make learning visible. Invite critique. Change course quickly when the data convinces you.

So what are the #Ramyfications
Build smaller tests with clearer outcomes. Thirty day wards, one clinic mornings, simple measures that matter to patients and staff.
Make reflection a ritual. After every test, write three lines. What surprised us, what scared us, what we change tomorrow.
Turn learners into mentors. Every person who tries the new thing trains the next person and records one tip for the library.
Speak with receipts. Publish short notes that show what you tried and what changed. Celebrate wins, own misses, state limits.
Use frameworks weekly, not yearly. RE AIM for the scorecard, CFIR for stubborn barriers, APEASE for hard choices.
Simulate before you scale. Fail safely in sandboxes, drills, and tabletop sessions, then move to live with confidence.
Treat new models as tools. Exciting, yes, but value must be proven in your context through measured outcomes, not promises.