Why Trust in Digital Health is Eroding
· Dr. Ramy Azzam
Post-COVID, everyone wanted to "transform" healthcare.
Billions were poured into virtual care, AI, remote monitoring, digital front doors, and for a moment, it felt like we’d finally cracked it. Innovation wasn’t just encouraged, it was urgent. The old resistance melted away. We all became digital believers.
But now, several years on, the digital health "revolution" looks… exhausted.
Why?
Because instead of building sustainable infrastructure, we built pilots. Instead of investing in deep transformation, we handed the mic to PowerPoint strategists with 3-hour certifications. And instead of being honest about outcomes, we got lost in vanity dashboards.
Welcome to the era of "Death by a Thousand Pilots." And the quiet erosion of credibility in digital health.
From Springboard to Swamp
Let’s be clear, pilots aren’t the enemy. A well-designed pilot tests assumptions, derisks investments, and engages stakeholders.
But in healthcare, pilots have become the endgame rather than the beginning. We’ve turned them into symbols of innovation, rather than steppingstones to scale. How many times have you heard:
"We’re running a pilot in one clinic before we decide."
"We’ve launched another MVP to test uptake."
"The Lessons Learned from this pilot is (bla bla bla). On to the next pilot"
Translation: We don’t want to commit. But we also don’t want to look like we’re not innovating. Let's rubber stamp this sh*t!
The Post-COVID Pandemic
The above is arguably a symptom of another pandemic, the overconfident underqualified digital health "expert". COVID cracked the gates open for an entire genre of self-proclaimed digital health experts armed with:
- Online courses,
- PM jargon ("synergize vertical KPIs with agile OKRs"),
- And a pie chart about "value creation"...
They parachuted into public health systems and private hospitals alike.
What they lacked in clinical understanding, they made up for in BS. They didn’t know the difference between a SOAP note and a spreadsheet, but they had frameworks. They couldn’t tell a KPI from an OKR, but they could diagram a transformation roadmap with six phases and five pillars, color-coded, of course.
While we developed vaccines for COVID, there are no vaccines for those, who are still lurking around leeching of terms like "revolution" "IOTs" and of course "AI", not only resulting in financial losses but also, patient losses.
 The post-covid digital health expert: Still uses Excel, hides it with edX certs and ChatGPT quotes.
The post-covid digital health expert: Still uses Excel, hides it with edX certs and ChatGPT quotes.
Garbage In, Garbage Out: The Data and Strategy Trap
Before transformation fails at the organizational level, it often fails at the data level. We’ve grown comfortable using the phrase “data-driven decision-making,” but few pause to ask: What’s driving the data?
The truth is, healthcare data is messy. It’s fragmented across outdated systems, riddled with inconsistencies, and full of contextless codes and incomplete records. ICD codes are misapplied. Free text is misinterpreted. A single patient can appear five different ways in five systems.
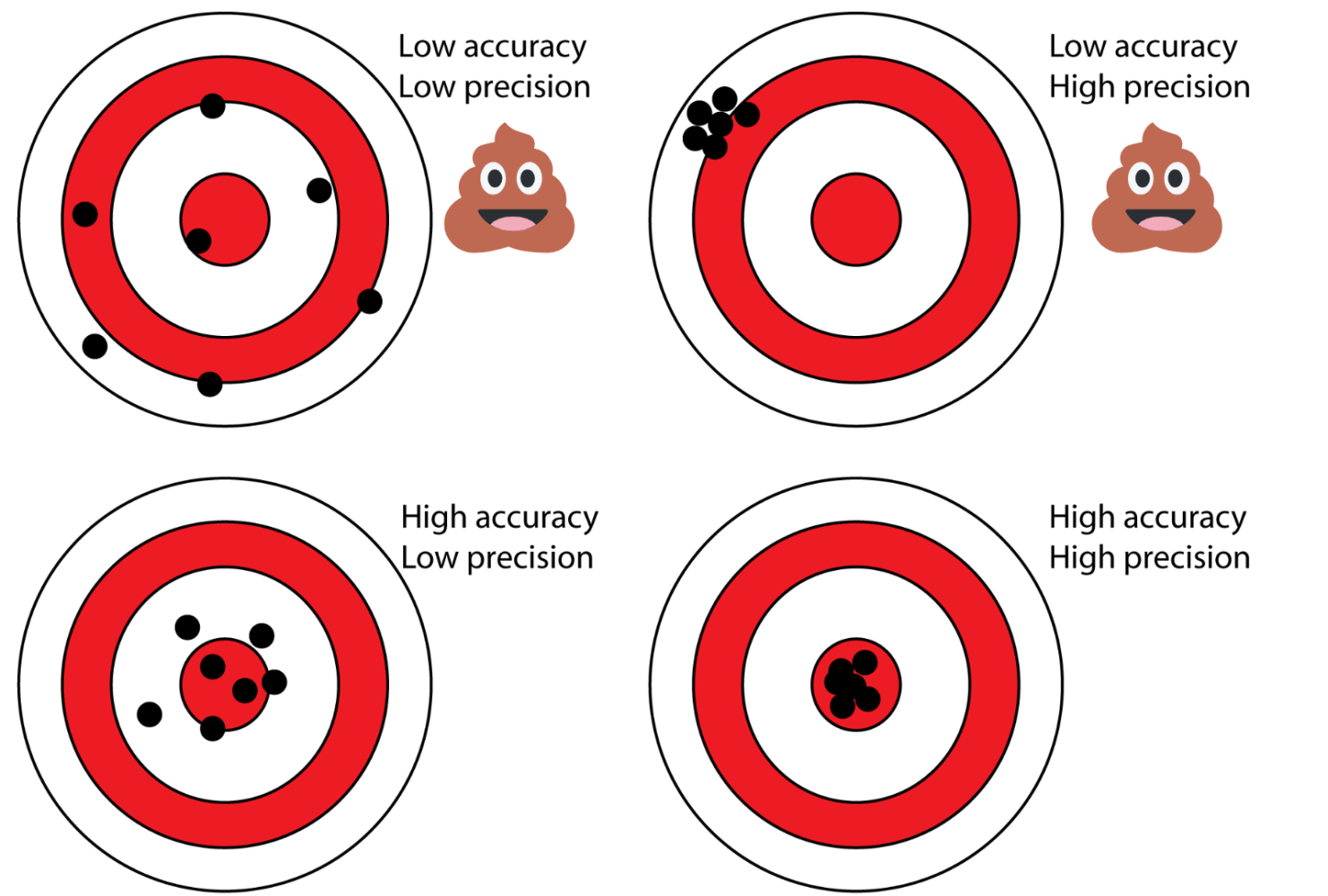
That’s the danger of GIGO: Garbage In, Garbage Out.
 Generated by ChatGPT: Garbage In -> Garbage Out
Generated by ChatGPT: Garbage In -> Garbage Out
Coined by George Fuechsel, an IBM technician and instructor, in the late 1950s and early 1960s. Fuechsel used the phrase to emphasize that the quality of output from computer systems depends entirely on the quality of the input data. In digital health, we’ve gone one step further. We feed in questionable data, layer on weak assumptions, and then base strategic decisions on what the dashboard tells us.
If you’ve been close to digital health deployment in recent years, you’ve probably seen this:
- Dashboards that show > 90% adoption (achieved by tweaking the denominator).
- Graphs of "engagement" (that are really just downloads, not even logins).
- Pilot "outcomes" declared as successful (without a single clinical metric).
- Magical High App Ratings (boosted by internal campaigns)... I've seen this first-hand, where in a townhall meeting, low ratings were attributed to bots from competitors... ??
And the result is "dashboard theatre", where optics outrun reality, and transformation becomes a KPI rather than a lived improvement.
But it’s not just the data. It’s the decision-makers too.
Enter the corollary: Garbage Professionals In, Garbage Strategy Out, or what I call GPS (Garbage Professionals Strategy). Name is a work in progress!
When digital transformation is led by those who lack clinical context, operational experience, or a grounding in healthcare realities, the result is strategy that looks good on paper (copied and pasted from ChatGPT without even bothering to change it from markdown to plain text), and that of course collapses under scrutiny.
The result? Policies optimized for false signals, tools nobody uses, programs nobody understands, metrics that are fabricated to look impressive, and a healthcare workforce left wondering why “digital transformation” feels more like digital confusion.
 The rise of garage digital health experts and their garbage dashboards
The rise of garage digital health experts and their garbage dashboards
What It’s Costing Us
We don’t talk enough about the opportunity cost of all this.
- Clinician Fatigue: Nurses and doctors are tired of trialing yet another app that doesn’t talk to the EMR or help with their actual work.
- Startup Burnout: Early-stage companies waste years jumping from pilot to pilot with no path to procurement.
- Patient Confusion: Every new tool introduces new logins, new workflows, new expectations.
- Strategic Stagnation: Leaders proudly announce "innovation pipelines" filled with pilots, yet core problems (access, equity, coordination) remain untouched.
And worst of all? It's eroding trust.
Every "transformation" that fails to deliver, chips away at the credibility of digital health.
 Garbage not only flatlines strategies but also flatlines patients.
Garbage not only flatlines strategies but also flatlines patients.
So How Can We Fix This?
Let’s Learn from Those Doing It Right. Take a page from Cleveland Clinic or NHSX (in its early days), where digital pilots were embedded into enterprise-wide strategies from day one.
They didn’t launch point solutions. They built integrated systems.
They didn’t treat pilots as science projects. They treated them as pre-scale simulations.
The key? They started with the end in mind.
Here’s a practical playbook for shifting from "pilot-heavy" to impact-ready:
1. Vet Ideas Before They’re Piloted
Not everything deserves a pilot. Just because it’s shiny and AI-enabled doesn’t mean it solves a real problem. Ask: Would we scale this if the pilot succeeds?
2. Start With the End in Mind
Define what success looks like, clinically, operationally, financially, before the pilot begins. Make sure those metrics are agreed upon across IT, clinical leadership, and procurement.
3. Build the Minimum Scalable Unit
Stop testing standalone features. Start piloting entire workflows that are designed to scale. If it only works in one clinic, it probably won’t work across the enterprise.
4. Fund for Scale, Not Just Experimentation
Pilots should come with a budget line for post-pilot integration, training, change management, and evaluation. Otherwise, we’re just funding theatre.
5. Be Honest About Failure
Failure isn’t the problem, failure theatre is. Share what didn’t work. Publish negative results. Normalize course correction. Your frontline teams will thank you.
Final Thought: Innovation Is Not a Performance
Healthcare doesn’t have a pilot problem. It has a commitment problem. We keep looking busy, launching shiny things, holding innovation summits. But the gap between proof of concept and proof of value remains gaping.
What we need now isn’t more dashboards, more frameworks, or more evangelists. We need executional discipline, shared accountability, and outcome-aligned leadership.
Because if we keep mistaking momentum for meaning, we’ll continue dying, not just by a thousand pilots, but by a thousand missed opportunities.
?? Seen this play out in your organization? Are you a recovering pilot champion yourself?